Down Syndrome is a chromosomal disorder linked with both an intellectual disability and a characteristic facial appearance. Health conditions vary person to person; and treatments often focus on the specific symptoms in each person. There is research about effective methods to edit genes – whether it be somatically or germline editing.
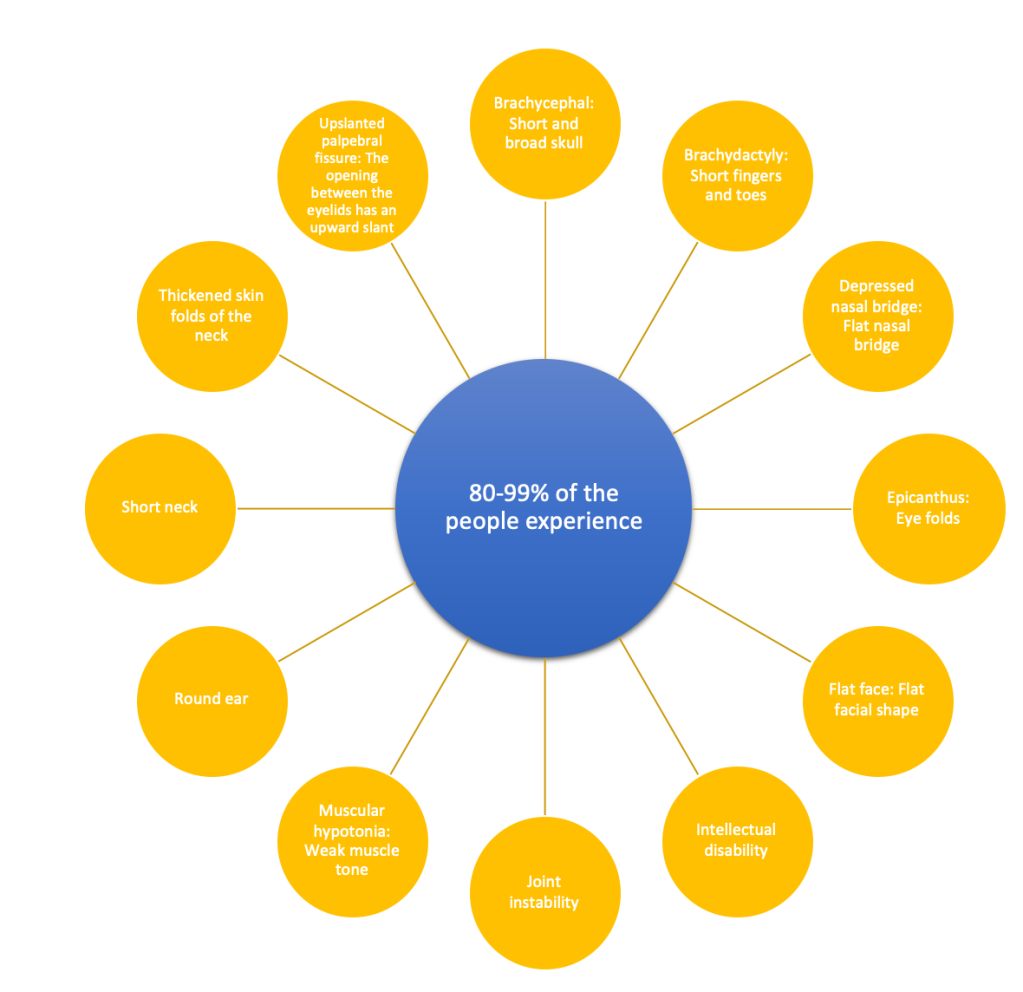
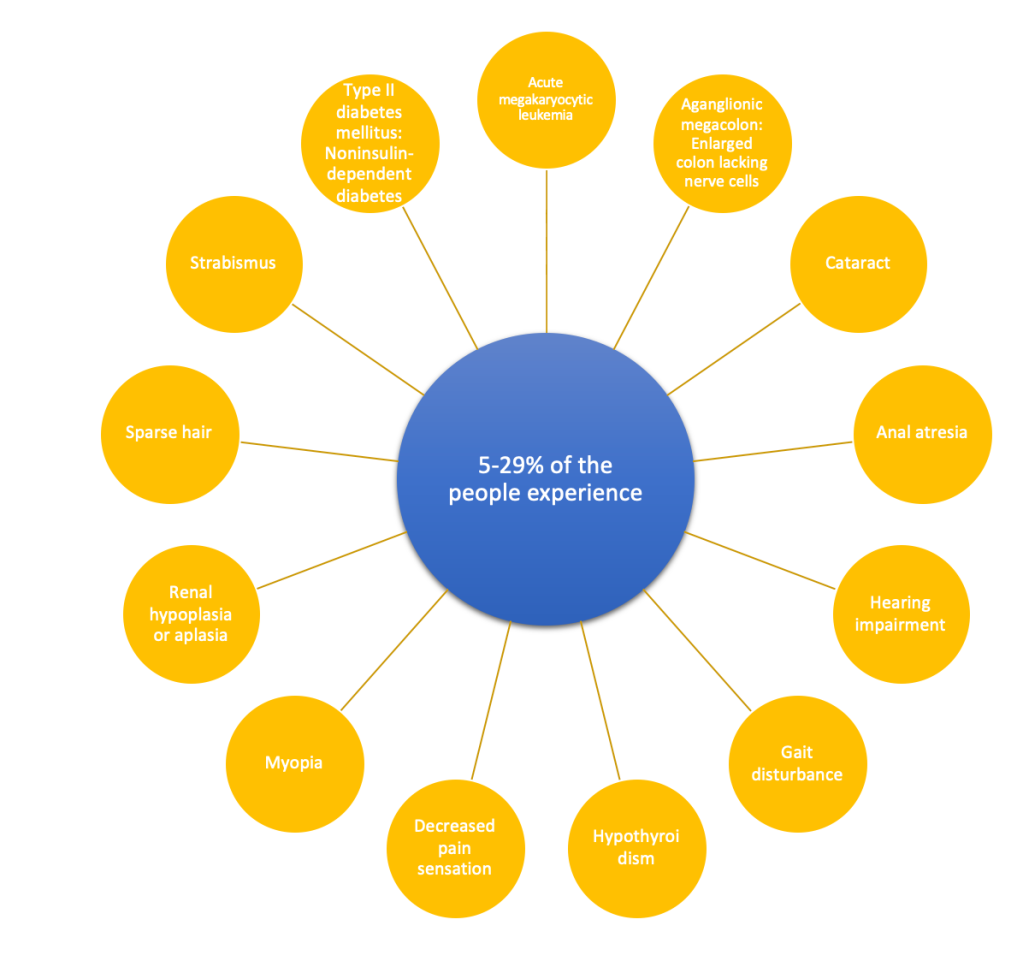
The symptoms that people with Down Syndrome experience vary. Children with Down Syndrome are more likely to develop chronic respiratory infections, middle ear infections and recurrent tonsillitis. Many have misalignment of two vertebrae in the neck – atlas and axis – this misalignment is called atlantoaxial instability. Individuals are also at risk of serious spinal cord injury due to overextension of the neck (Down Syndrome). Most children experience a developmental delay; they are slower in turning over, sitting and standing. This is mostly an effect linked with the child’s weak muscle tone. Speech and language development could also take longer. Adults with Down Syndrome have an increased risk of developing early onset Alzheimer disease. Although Alzheimer is a disorder that affects people older in age, almost half of adults with Down Syndrome develop this by age 50. People with Down Syndrome are more prone to immune disorders. This is caused by abnormalities in their immune systems. They have increased susceptibility to developing autoimmune disorders, some cancers and diseases like pneumonia and other respiratory issues (Down Syndrome – Gene – NCBI).

There are three main causes of Down Syndrome (Chromosome 21 Ring). The first is “complete” trisomy 21. It is caused by an extra chromosome 21 in all cells of the person that is affected. The chromosome 21 pair do not separate during the formation of the egg or sperm. This is called “nondisjunction”, the cause of “nondisjunction” is unknown as of now. It is alluded that as women age this happens more often. However, research suggests that it is not caused by anything a parent may do before or during a pregnancy as well as any environmental factors. In most cases the extra copy of chromosome 21 comes from the mother in the egg. In less than 5% of Down Syndrome cases – the extra copy comes through the sperm. In the remaining cases, the mutation occurs as the embryo grows. When an egg with 2 copies of chromosome 21 meets a normal sperm with only 1 copy of chromosome 21, the embryo has 3 copies of chromosome 21, rather than just 2 (Down Syndrome). The extra third chromosome is copied into every cell of the child which results in Down Syndrome.
The second cause is mosaic trisomy 21. This type of mutation accounts for only about 1-2% cases of Down Syndrome. This means that only some cells in the body have an extra chromosome 21. It is caused when a fertilized egg has the right number of chromosomes, but because of an early cell division error in the embryo development stages, some cells get an extra chromosome 21. People with mosaic trisomy 21 have 46 chromosomes in some cells and 47 in others. As a result, the prominence of Down Syndrome, its feature and the severity may vary (Chromosome 21 Ring).
The third type is translocation trisomy 21 which is present for an estimated 3-4% cases of Down Syndrome. Cells in people that have this form of trisomy 21 contain 46 chromosomes; but there is extra chromosome 21 material translocated or “attached” or “stuck” onto another chromosome. For the parents of a child with Down Syndrome caused by translocation, the chances of having more children with Down Syndrome are increased. This is because one of the two parents may be a carrier of a balance translocation; which occurs when a piece of 1 chromosome breaks off and attaches to another. Albeit, not all parents of babies with translocation trisomy 21 have a translocation (Chromosome 21 Ring).
One risk factor for Down Syndrome is advancing maternal age- as a woman gets older, their eggs have a greater chance of faulty chromosomal division. Having a child with Down Syndrome increases after the age 35. That being said, most children with Down Syndrome are born to women under 35 because younger women have more children. In fact, they give birth to 80% of the children with Down Syndrome. There has been very little to almost no research proving behavioral activity or environmental factors to cause Down Syndrome (About Down Syndrome).
Down Syndrome’s annual prevalence rate is about 1 in 800 to 1 in 1000 newborns. Yearly, there are 5,300 babies born with Down Syndrome in the US. The National Down Syndrome Society says that there are approximately 340,000-400,000 people with Down Syndrome (Presson, Angela P, et al). In a sample of 75 children with Down Syndrome; there were 42 males and 33 females. The sex ratio was 1.30; there was an excess of males in the referred population (A;, Verma RS;Huq). This is because more males with Down Syndrome are born to younger mothers, while mothers older in age had more females with Down Syndrome. The lifespan for people with Down Syndrome has increased greatly over years for people with Down Syndrome. In 1983, the life expectancy was 25 years. Individuals with Down Syndrome can now expect to live more than 60 years, but it differs based on the intensity of the health problems they experience (Data and Statistics on Down Syndrome).
Diagnosis and testing for Down Syndrome can be done both before and after the baby is born. To confirm Down Syndrome before birth, many prenatal tests can be done. An amniocentesis is when a needle is inserted through the abdominal wall into the amniotic sac. A sample of amniotic fluid is drawn out then tested for any diseases. Chorionic villus sampling or CVS also called chorionic villus biopsy is a prenatal test that involves taking a tissue sample from the placenta to test for chromosomal abnormalities and other genetic disorders (What Causes Down Syndrome).
If a child is not prenatally diagnosed, then testing usually begins at birth based on your child’s physical appearance. Once a diagnosis is made, extra testing is used for clinicians to understand how Down Syndrome may affect the baby. Genetic testing, which uses a saliva sample to identify DNA, can be used for further testing. As well as blood tests, they help determine drug usage and effectiveness, biochemical diseases, and organ function. Others include X-rays, MRIs, CT scans, and EOS imaging; which is an imaging technology that creates 3-D models using planar images. EOS images are taken while one is upright or in a standing position; not like CT scans, where they lay down. This change in position helps by enabling improved diagnosis due to weight-bearing positioning (Down Syndrome: MedlinePlus Genetics).
Treatments for Down Syndrome are not a remedy for the disease, but are precautions to help keep it controlled. Early intervention services like assistive technology, audiology, speech and language services, counseling and training for a family, medical services, nursing services, nutrition services, occupational therapy, physical therapy, psychological services, quality educational programs and a stimulating home environment. The goal of these types of training is to boost cognition by improving learning, memory, and speech. Other treatments depend on the specific health problems or complications present in each person. All newborns with Down Syndrome have their heart checked with an electrocardiogram and an echocardiogram because 40-60% babies born with Down Syndrome have some form of a heart defect (Down Syndrome Mayo Clinic). Infants with Down Syndrome are referred to pediatric cardiologists for regular check-ups or pediatric cardiac surgeons for early surgical intervention (The Children’s Hospital of Philadelphia). It is also recommended to get a thyroid test every year, since many have low thyroid levels. Many others could require surgical correction.
Scientists are hopeful that with new technology, Down Syndrome could be cured. Researchers have identified two important gene locations linked to Down Syndrome. The Olig1 and Olig2; reducing the activity of these two genes in mice designed to imitate the disorder helped correct brain activity in them. This research suggests that Olig1 and Olig2 inhibitors may have a therapeutic role for people with Down Syndrome. Zygmunt Galdzicki says “We hope these findings will lead to better strategies for early intervention […]” (Singer, Emily).
There are two main ways that gene therapy could treat Down Syndrome. It could be used somatically, making changes to an individual’s genome that cannot be inherited. Somatic avenues for treating Down Syndrome have the potential to “cure” conditions like the loss of nerve cells which leads to weak musculature. But there are difficulties in areas such as; defining the precise genes responsible for some conditions that are present in people with Down Syndrome and being able to both safely and efficiently target the genes without mistakes. In 2014, geneticists from the University of Massachusetts Medical School were able to “turn off” the extra chromosome 21 that causes Down Syndrome (Lennon, Annie). They added an RNA gene known as X-inactive specific transcript or XIST to human stem cells. When XIST was inserted onto the extra chromosome in cells that have the trisomy 21 mutation – they created a buildup of RNA that coated the copy of chromosome 21 and shut it down. But, for this to completely eliminate Down Syndrome, the procedure would have to be done on most or all cells in a body. This is the reason germline treatments are more attractive as fewer cells can be treated at once.
Germline treatments are used for making changes to the genomes of very early embryos that may be inherited. In 2017, Scientists in China used CRISPR/Cas9 technology to edit and eliminate sex chromosomes and autosomes in culture cells, embryos and in vivo tissues (Lennon, Annie). They were able to eliminate the copy of chromosome 21 using CRISPR, but not in embryos. They were able to conclude that a single autosomal deletion would lead to embryonic lethality and that the CRISPR/Cas9 system should be used to limit chromosome functionality, instead of deletion.
Down Syndrome is a genetic anomaly that results from abnormal division involving chromosome 21. As children with Down Syndrome grow, they are at a greater risk for certain medical problems. Existing medications can help alleviate the conditions; therapy can help with cognitive skills, communication and social skills and can also help with physical developmental delay. Advancing biomedical discoveries are close to “curing” the disorder. There is nothing down about it!
Bibliography
A;, Verma RS;Huq. “Sex Ratio of Children with Trisomy 21 or Down Syndrome.” Cytobios, U.S. National Library of Medicine, pubmed.ncbi.nlm.nih.gov/2960497/.
About Down Syndrome. Genome.gov, http://www.genome.gov/Genetic-Disorders/Down-Syndrome.
The Children’s Hospital of Philadelphia. “Trisomy 21 (Down Syndrome).” Children’s Hospital of Philadelphia, The Children’s Hospital of Philadelphia, 31 Mar. 2014, http://www.chop.edu/conditions-diseases/trisomy-21-down-syndrome.
Chromosome 21 Ring. NORD (National Organization for Rare Disorders), rarediseases.org/rare-diseases/chromosome-21-ring/.
Data and Statistics on Down Syndrome. Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 5 Dec. 2019, http://www.cdc.gov/ncbddd/birthdefects/downsyndrome/data.html.
Down Syndrome – Gene – NCBI. National Center for Biotechnology Information, U.S. National Library of Medicine, http://www.ncbi.nlm.nih.gov/gene/?term=down+syndrome.
Down Syndrome. Genetic and Rare Diseases Information Center, U.S. Department of Health and Human Services, rarediseases.info.nih.gov/diseases/10247/down-syndrome.
Down Syndrome. Mayo Clinic, Mayo Foundation for Medical Education and Research, 8 Mar. 2018, http://www.mayoclinic.org/diseases-conditions/down-syndrome/symptoms-causes/syc-20355977.
Down Syndrome: MedlinePlus Genetics. MedlinePlus, U.S. National Library of Medicine, 8 Sept. 2020, medlineplus.gov/genetics/condition/down-syndrome/.
Growth Charts for Children with Down Syndrome. Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 5 Dec. 2019, http://www.cdc.gov/ncbddd/birthdefects/downsyndrome/growth-charts.html.
Lennon, Annie. “Can We Cure Down’s Syndrome with Gene Therapy?: Genetics And Genomics.” LabRoots, Labroots, 20 Dec. 2019, http://www.labroots.com/trending/genetics-and-genomics/16411/cure-down-s-syndrome-gene-therapy.
Presson, Angela P, et al. “Current Estimate of Down Syndrome Population Prevalence in the United States.” The Journal of Pediatrics, U.S. National Library of Medicine, Oct. 2013, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4445685/.
Singer, Emily. “The Genes Behind Down Syndrome.” MIT Technology Review, MIT Technology Review, 2 Apr. 2020, http://www.technologyreview.com/2010/07/19/201973/the-genes-behind-down-syndrome/.
What Causes Down Syndrome? Eunice Kennedy Shriver National Institute of Child Health and Human Development, U.S. Department of Health and Human Services, http://www.nichd.nih.gov/health/topics/down/conditioninfo/causes.
Zemel, Babette S, et al. “Growth Charts for Children With Down Syndrome in the United States.” Pediatrics, U.S. National Library of Medicine, Nov. 2015, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC5451269/.
